History:
53yo female with DM and COPD presents to your ED approximately 20 minutes after stepping on what she believes to be a toothpick, however since this foreign body is now trapped beneath the skin of the sole of her foot (at least according to her), she is actually not certain precisely what she stepped on. She was barefoot at the time of the incident and offers no other complaints.
Examination:
AFVSS
Extremity exam: small puncture wound on plantar surface of forefoot near the heads of the 1st and 2nd metatarsals. Beneath the puncture wound a soft mass measuring approximately 2cm in diameter with mild tenderness is palpable. No erythema, warmth, fluctuance, crepitance or purulence.
Emergency Department Course:
The patient was treated with oral analgesia and sent to radiology for plain radiographs of the foot to evaluate for evidence of a retained foreign body.
Radiographs:



The images were interpreted by radiology as negative for a retained foreign body. A bedside ultrasound examination was performed because the history and exam so strongly suggested a retained foreign body, one that might be organic and therefore not visualized with plain radiographs.
Ultrasound Examination of the Foot:
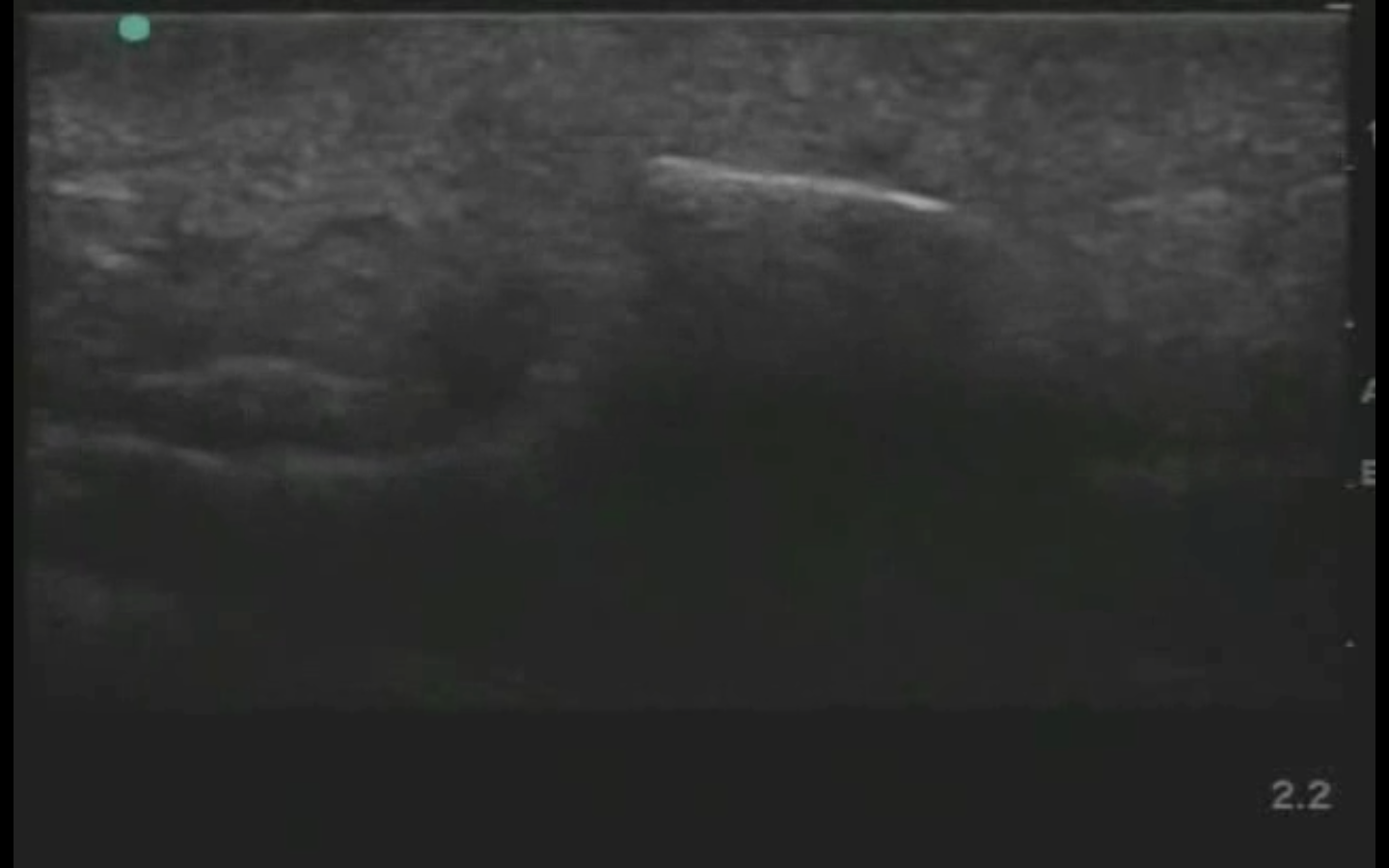
Using a high frequency linear transducer with the a musculoskeletal exam setting, the following image was obtained:

In the near field of the image you see a hyperechoic line with posterior acoustic shadowing surrounded by indistinct, heterogeneous soft tissue that lacks a normal, organized architecture. These findings are consistent with a retained foreign body.
Procedure:
You then perform a field block with lidocaine 1% with epinephrine, and make a small incision utilizing a #15 blade scalpel. Using US-guidance you are able to retrieve the foreign body with a hemostat.

Conclusion:
The patient is elated that you were able to successfully remove this broken piece of a toothpick (the type that goes in a club sandwich, which she now recalls eating for lunch yesterday). You put her on prophylactic antibiotics and discharge her home.
Take Home Points:
1. Plain radiographs are an inferior imaging modality to US for the detection or organic foreign bodies.
2. A recent systematic review with meta-analysis published in Academic Emergency Medicine found POC US to be moderately sensitive and highly specific for the identification of FB’s.
Davis_et_al-2015-Academic_Emergency_Medicine
3. Posterior acoustic shadowing may be the only reliable US feature to identify a FB as not all FB’s are intensely hyperechoic. If you identify abnormal shadowing in an area where the pt has symptoms of a retained FB you are likely looking at the FB.
